

Introduction
Acute arterial embolism and thoracic outlet syndrome (TOS) associated with cervical rib deformity are uncommon clinical entities. Cervical rib deformities occur in approximately 0.6% of the population and are frequently asymptomatic.(2) However, in rare instances, this anomaly can result in severe vascular complications, such as subclavian artery aneurysm. Timely diagnosis and prompt surgical intervention are crucial to prevent potentially life-threatening complications, including limb ischemia and mortality. This report presents the case of a 38-year-old patient diagnosed with thoracic outlet syndrome complicated by acute arterial embolism. Surgical intervention was successfully performed, leading to the restoration of normal blood flow and substantial improvement in the patient’s condition.
Case Presentation:
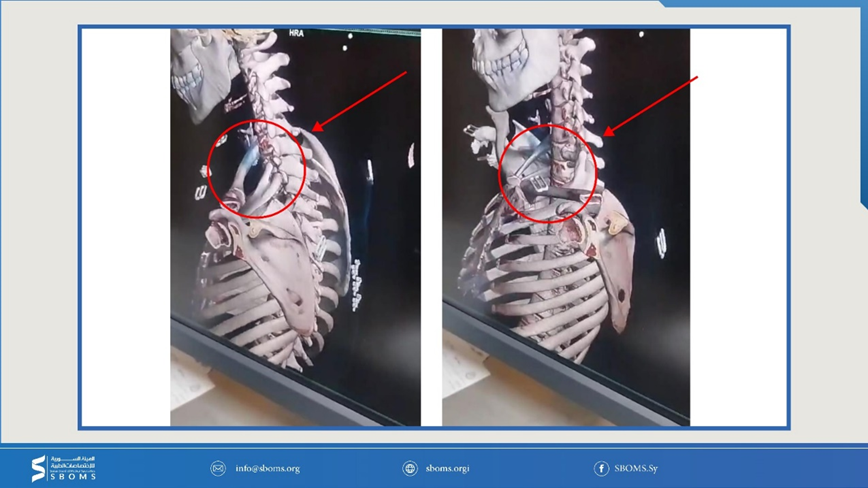
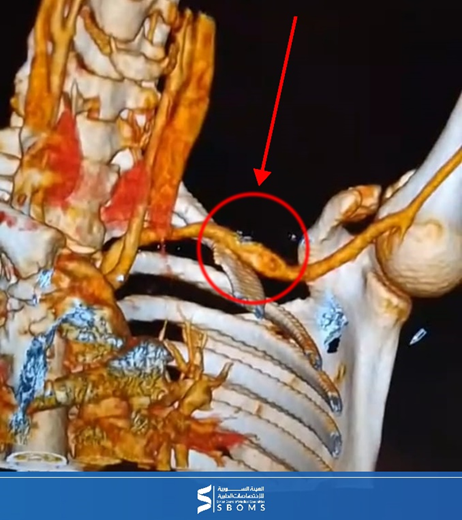
A 38-year-old patient presented to the emergency department of the Specialized Surgical Hospital in Idlib with complaints of numbness and severe pain in the upper left limb, along with a sensation of coldness. The medical team conducted the necessary diagnostic evaluations, including contrast-enhanced computed
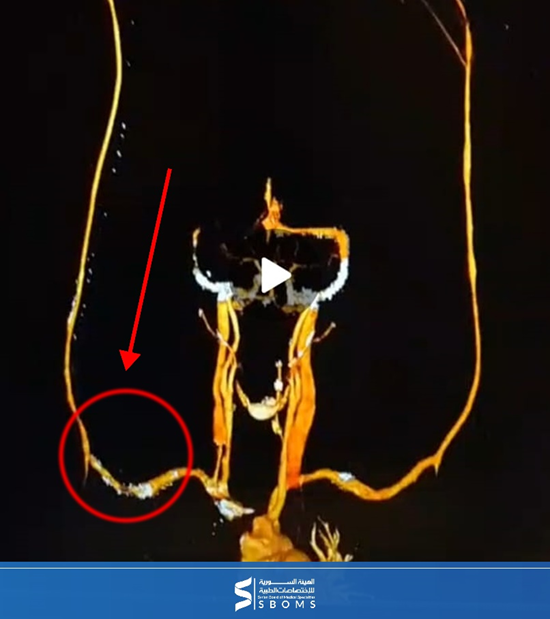
tomography, which revealed a significant blockage in the brachial artery. This blockage was attributed to cervical rib compression on the subclavian vessels, leading to an abnormal dilation (aneurysm)
in the subclavian artery.
Surgical management:
Due to the severity of the condition, an immediate decision was made to proceed with surgical intervention. The procedure was performed in two stages:
First Stage:
Procedure:
- The embolus was removed using a Fogarty catheter to restore blood supply to the affected upper limb.
- The thrombosis was successfully extracted, leading to immediate improvement in blood flow and the restoration of vitality to the limb.
Second Stage:
- This stage involved preparing the patient for a more extensive surgical procedure, which included the removal of the cervical rib causing compression on the blood vessels. Additionally, biopsies were taken from the anterior and middle scalene muscles to alleviate pressure on the neurovascular bundle. The subclavian aneurysm was excised beneath the clavicle, and a reinforced artificial graft was placed with an end-to-end anastomosis between the graft and the subclavian artery to ensure the continuous blood supply to the affected limb, following the damage caused by the cervical rib compression.
- Postoperative ultrasound examination demonstrated adequate and effective blood flow, confirming the success of the surgery and the complete restoration of normal vascular function.

Conclusion:
This condition highlights the importance of early diagnosis and immediate surgical intervention to treat acute arterial embolism caused by cervical rib deformity. The two-stage surgical approach, which combined embolic removal and deformity correction, has been shown to be effective in restoring blood flow and preventing serious complications.
The condition indicates that thoracic outlet syndrome should be suspected in patients with upper limb ischemia with neurological symptoms. Cervical rib deformities can lead to serious vascular complications that require rapid intervention from various specialties. Two-stage surgical intervention provided immediate limb rescue, with the underlying deformity planned to be corrected, and the prosthesis ensured long-term vessel stability.
Thoracic Outlet Syndrome
Acute arterial embolism and thoracic outlet syndrome (TOS) associated with a cervical rib are rare but potentially serious conditions that can result in complications such as limb ischemia and, in severe cases, the loss of fingers or limbs. Radiological studies estimate the prevalence of cervical ribs in less than 1% of the general population, though research suggests this rate can vary widely, from 0.58% to 6.2%, depending on the population studied.(1) While many individuals remain asymptomatic, in some cases, these anatomical anomalies exert pressure on neurovascular structures, leading to significant morbidity.
Clinical Symptoms and Diagnosis
Patients with cervical ribs may present with upper limb ischemia and neurological symptoms, such as pain, tingling, or weakness, resulting from compression of the brachial plexus or subclavian artery. Diagnosis typically involves imaging studies, such as X-rays or MRIs, to identify the presence of a cervical rib and evaluate its impact on surrounding anatomical structures. The presence of a cervical rib can contribute to the development of thoracic outlet syndrome (TOS), characterized by symptoms including a diminished radial pulse and nerve deficits when the arm is positioned in certain ways, such as during abduction or elevation.(2)
Surgical Management
The treatment of acute arterial embolism and thoracic outlet syndrome due to cervical rib involvement often requires a multidisciplinary approach, typically involving both vascular and thoracic surgeons.(3) Urgent surgical intervention is essential to restore blood flow and prevent ischemic damage to the affected limb. A two-stage surgical approach is commonly employed:
- Immediate Limb Rescue: The first phase focuses on restoring vascular integrity, often through thrombectomy to remove blood clots and reestablish blood flow to the affected limb.
- Anatomical Correction: The second phase involves the resection of the cervical rib to alleviate pressure on the neurovascular structures, essential for long-term management and to prevent recurrence of symptoms.
The Importance of Early Diagnosis
Early diagnosis and prompt intervention are crucial in preventing severe complications associated with cervical rib deformities. The risk of ischemic damage rises significantly with delayed treatment. Case reports underscore the importance of maintaining a high index of suspicion for thoracic outlet syndrome in patients presenting with upper limb ischemia, particularly when neurological symptoms are also present. Successful management of such cases highlights the necessity of comprehensive vascular evaluation and the effectiveness of surgical interventions in addressing both acute and chronic complications arising from cervical rib-associated thoracic outlet syndrome.(4)
Disclaimer:
This case was managed at the Specialized Surgical Hospital in Idlib supported by the Medical Association of Syrian Expatriates SEMA, under the supervision of Dr. Ali Al-Saeed Member of the Scientific Council of Vascular Surgery, and the resident doctor Mohammed Al-Junaid in vascular surgery at the Syrian Board of Medical Specializations SBOMS.
References
- Spadliński Ł, Cecot T, Majos A, Stefańczyk L, Pietruszewska W, Wysiadecki G, et al. The Epidemiological, Morphological, and Clinical Aspects of the Cervical Ribs in Humans. Vol. 2016, BioMed Research International. 2016.
- Brian Fliegel AE, Menezes Affiliations RG. Anatomy, Thorax, Cervical Rib. 2024.
- Köksal V. Cervical rib which resembles original thoracic rib presenting with thoracic outlet syndrome (TOS): Literature review with a case report. International Journal of Morphology. 2019;37(4).
- Roy S, Jain N, Narang E, Singh J. Cervical Rib: A Rare Differential of a Supraclavicular Mass. Vol. 101, Ear, Nose and Throat Journal. 2022.
- Roos DB. Thoracic outlet syndrome is a multidimensional compression syndrome of the upper extremity. Clin Orthop Relat Res. 1986;(207):6-22.
- Wilbourn AJ. The thoracic outlet syndrome is overdiagnosed. Arch Neurol. 1990;47(3):328-330.
- Sheth RN, Belzberg AJ. Diagnosis and treatment of thoracic outlet syndrome. Neurosurg Clin N Am. 2001;12(2):295-309.