

Introduction
Aortic coarctation is a rare congenital defect that disrupts blood flow, leading to hypertension in the upper body and reduced circulation to the lower extremities. This condition is a significant cause of treatment-resistant hypertension in young individuals and may remain undiagnosed until adulthood, increasing the risk of cardiovascular complications.
This report presents the case of a 20-year-old male who underwent the first successful catheter-based expansion of aortic coarctation in Idleb – Northwest Syria. The vascular surgery team at the Specialized Surgical Hospital in Idlib performed this procedure, significantly improving the patient’s health and mitigating disease complications.

Case Presentation
Patient Information
- Age & Gender: 20-year-old male
- Presenting Symptoms: Severe, treatment-resistant hypertension and intermittent claudication in both lower limbs, significantly affecting his quality of life.
- Medical History: No chronic illnesses or previous surgical interventions.
Clinical Examination
- Consciousness Level: The patient was alert and oriented.
- Vital Signs: Blood pressure of 180/110 mmHg in the upper limbs.
- Cardiovascular Examination: Absence of peripheral pulses in both lower extremities.
Radiological and Laboratory Diagnosis
- Transthoracic Echocardiography: Revealed high-velocity blood flow at the coarctation site with increased vascular resistance.
- Renal Function Tests: Normal, indicating no direct impact on renal perfusion.
Treatment Decision and Surgical Intervention
- Therapeutic Options Discussed:
- Open Surgery: Resection of the stenotic segment with end-to-end anastomosis.
- Catheter-Based Expansion with Stent Placement: A minimally invasive approach offering faster recovery and reduced complication risk.
After a comprehensive evaluation and considering the patient’s preference, the decision was made to proceed with catheter-based expansion and stent placement.
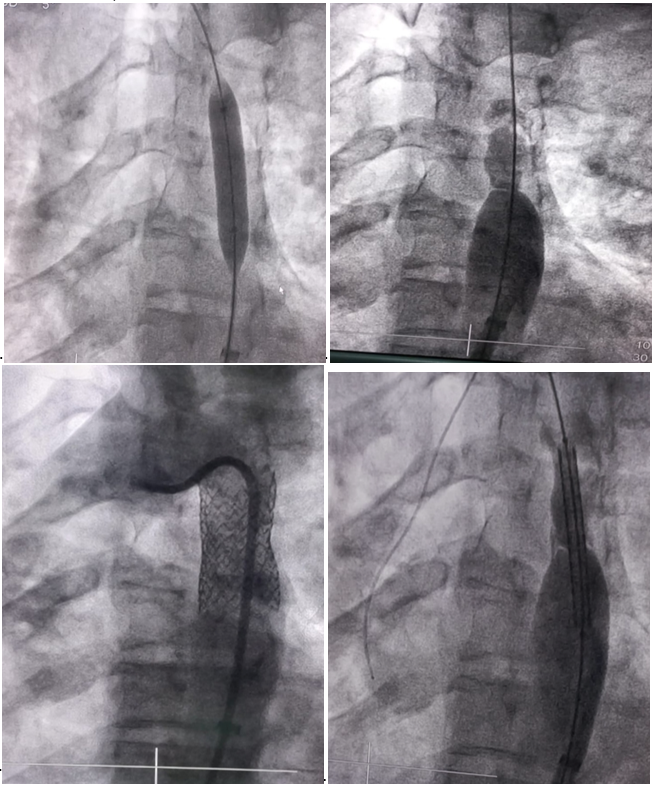
Intervention:
The procedure was performed under local anesthesia with continuous cardiac monitoring.
A BeGraft Aortic Stent was deployed to expand the narrowed segment and restore normal blood flow.
Immediate angiographic imaging confirmed successful expansion.
Post-Procedure Outcomes
Immediate Monitoring
- Significant improvement in blood flow.
- Blood pressure reduction to 110/75 mmHg, indicating a successful response.
- Restoration of peripheral pulses in the lower limbs and improved ambulation.
- Stable vital signs without immediate complications.
- The patient was discharged after 24 hours in good general condition with follow-up recommendations.
Long-Term Follow-Up
- Regular blood pressure monitoring and cardiovascular assessments.
- Imaging studies every 6-12 months to ensure stability and detect potential restenosis.
- Lifestyle modifications and adherence to medical therapy.
- Scheduled follow-ups with a vascular surgery specialist.
Disease Overview: Aortic Coarctation in Adults
Pathophysiology
Aortic coarctation is a congenital anomaly characterized by narrowing of the aortic isthmus, the segment between the left subclavian artery and the ductal attachment in the descending aorta. This narrowing leads to:
- Pre-Coarctation Hypertension: Affects the head, upper limbs, and cerebral arteries.
- Post-Coarctation Hypoperfusion: Affects the lower limbs, kidneys, and intestines.
- Collateral Circulation Development: Leads to intercostal artery enlargement, visible as rib notching on imaging.
- Increased Left Ventricular Afterload: Potentially resulting in long-term heart failure.
Clinical Manifestations in Adults
- Severe, treatment-resistant hypertension.
- A significant blood pressure gradient between upper and lower limbs (>20 mmHg).
- Weak or absent femoral pulses with a delay relative to the brachial pulse.
- Intermittent claudication due to reduced lower limb perfusion.
- Headaches and epistaxis resulting from uncontrolled hypertension.
- In untreated cases, complications may include aortic aneurysm, rupture, or stroke.
Diagnostic Approach
- Blood Pressure Measurement: Detects upper-lower limb discrepancy.
- Chest X-ray: Shows rib notching due to collateral vessel enlargement.
- Echocardiography (Transthoracic or Transesophageal): Assesses flow turbulence and narrowing severity.
- CTA or MRA: Defines the coarctation extent and guides treatment planning.
- Cardiac Catheterization: Measures pressure gradients and evaluates the need for intervention.
Treatment Options
- Catheter-Based Stenting: The first-line treatment for most adult cases.
- Open Surgical Repair: Reserved for complex cases or aneurysmal aortic involvement.
- Long-Term Follow-Up: Essential for blood pressure control and vascular complication prevention.
Prognosis
With appropriate intervention, patients can achieve normal life expectancy, provided they undergo regular blood pressure and cardiovascular monitoring. If left untreated, complications such as heart failure, stroke, or aortic rupture can occur.
A Medical Breakthrough Offering Hope
This achievement represents a significant advancement in interventional vascular surgery in Northwest Syria, particularly in Idlib. It showcases the available medical capabilities despite existing challenges, providing new hope for patients with complex vascular diseases. Furthermore, it underscores the importance of medical progress in the region, reinforcing patient trust in local healthcare services and expanding access to specialized treatment.
Conclusion
This case highlights the importance of early diagnosis and timely intervention in adult aortic coarctation. Catheter-based expansion is an effective, minimally invasive treatment with a favorable safety profile, improving patients’ quality of life and reducing long-term complications. Regular blood pressure monitoring and cardiovascular evaluations are essential for ensuring long-term treatment success.
Acknowledgment
This procedure was performed at the Specialized Surgical Hospital in Idlib under the supervision of a team of vascular surgeons: Dr. Wael Habib (Chair of the Scientific Council for Vascular Surgery at SBOMS), Dr. Ali Al-Saeed (Council Member), and Dr. Mohammad Al-Junaid (Vascular Surgery Resident). This report has been published with the patient’s and his family’s consent for educational purposes.
Edited by: Dr. Fayez Orabi
References