
Pathological history:
A 57-year-old patient at Al-Quds Hospital, supported by Hand in Hand, came with a rash on the legs and arms with hematuria and hemoptysis 4 days ago. He was interviewed by Dr. Ahmed Ghazal, a resident doctor in Internal Medicine. A review of the patient’s medical history shows that he has type II diabetes, arterial hypertension, cardiac ischemia, and newly discovered chronic renal disease with proteinuria. Upon closer examination of the patient’s story, it was found that he suffers from chest pain and respiratory dyspnea degree III in addition to painless hematuria and hemoptysis.
It was also revealed by more seeking that the patient had black or tarry defecation

Clinical examination:
- Chest listening showed faint respiratory sounds in the right lung.
- Itchy, painless purpura localized especially on the lower extremities and on the extensor surfaces of the hands.
- Vital signs upon arrival are as follows: arterial pressure 90/60, pulse 70/min, blood oxygen saturation 92%, and random blood sugar 400 mg/dL.
Initial clinical impression:
The Initial clinical impression was systemic vasculitis supervised by Dr. Wassim Zakaria, the Supervising Internal Medicine Specialist.
Radiological and laboratory investigations:
radiological and laboratory investigations were requested to confirm the diagnosis.
X-ray: A simple chest scan was performed, which showed enlargement of the cardiothoracic hairy with a right pleural effusion.
Electrocardiogram: The ECG showed poor development of the R wave.
Laboratory tests: Preliminary laboratory tests showed the presence of renal insufficiency with elevated inflammatory indicators with the presence of hematuria proteinuria in a random urine sample of 1275g, and the lab analyzes did not reveal any disorder in platelets or coagulation factors, which increased the suspicion of vasculitis
- ESR 98
- CRP 88
- Creatinine 3.2
- Urea 120
- Hgb 14
- Platelet 166.000
- – WBC 12000
- INR 1.17
- – PTTK 33

Urinary system echography:
An ultrasound of the urinary system was ordered and was normal which excluded the presence of obstruction.
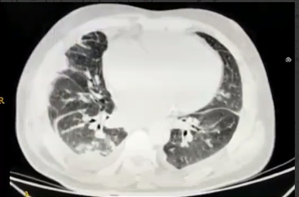
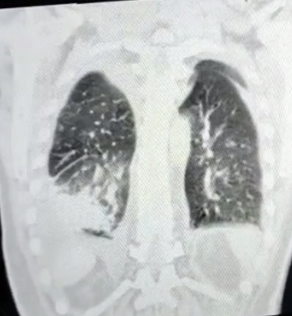
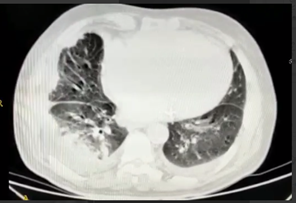
Computed tomography:
: A chest CT scan was ordered to investigate the cause of pleural effusion, and the CT showed the presence of pervasive condensation at the base of the right lung as well as effusion, with a differential diagnosis of tumor, pneumonia, or atelectasis.

Management and follow-up:
Dr Ahmed Ghazal admitted the patient to the intensive care unit to complete the study and treatment, where he developed a deterioration in kidney functions, which necessitated a kidney consultation and additional analyzes were requested in order to narrow the diagnosis more, where some immunological and serological analyzes were requested cANCA, pANCA, C3, C4, anti-GBM, hepatitis B – C viruses, and the result was all normal.
After consulting the Pulmonologist and Nephrologists and ruling out other causes of small vessel inflammation, a diagnosis of Henoch-Schonlein purpura caused by pneumonia with hematuria and epistemic defecation was made.
Treatment with corticosteroids was started intravenously with intravenous antibiotics and good hydration with strict blood glucose monitoring and daily follow-up of kidney function and electrolytes, and days after starting treatment, creatine numbers decreased from 6.5 to3.2 and no urgent dialysis session was required for the patient, the patient was transferred to the ward in the hospital to complete treatment and was discharged after 15 days in good health with clinical and radiological improvement and the return of laboratory tests their normal or basal levels.
Discussion:
Henoch-Schonlein purpura is rare in adults and is more common in children in 90% of cases and is the most common type of inflammation of the small vessels where it affects veins and capillaries, usually preceded by upper respiratory infection (in this patient the infection was lower), and then manifests as particularly palpable purpura on the lower extremities, arthritis, abdominal pain, usually bloody defecation, and hematuria.
Other causes of vasculitis are usually ruled out by skin or kidney biopsy.
The course of the disease is usually self-limiting and good hydration and symptomatic treatment are sufficient.
In mixed cases, such as in this patient, corticosteroids may be used in treatment.
What is distinctive in this case is that the patient is exhausted by diseases – two associated diseases at the same time, with pneumonia and Henoch-Schonlein purpura, which made the diagnosis confusing at first, as small vasculitis (Wagner – Microscopic – Churg and Strauss) was thought of, which is characterized by the presence of renal and pulmonary injury usually, and these cases were excluded by conducting laboratory analyzes which were negative. It was published several articles in the medical literature that infection with some types of pneumonia, such as mycoplasma, maybe cause Henoch-Schonlein purpura. In this patient’s case, the manifestation of pneumonia was in the form of hemoptysis, which is rare for Henoch-Schonlein purpura to manifest hemoptysis.
The explanation for the deterioration of kidney function in the presence of pre-existing diabetic nephropathy in the patient is due to pneumonia and fluid deficiency with no relation to the Henoch-Schonlein purpura.
References:
- https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Henoch-Schönlein-Purpura-HSP , Henoch Schönlein Purpura (HSP)
- https://pubmed.ncbi.nlm.nih.gov/26862316/ Mycoplasma pneumoniae as a trigger for Henoch-Schönlein purpura in children, Elżbieta Kuźma-Mroczkowska
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664214/ Henoch-SchöNlein Purpura in Adults، María José López Meiller,