

Case History:
The 17-year-old patient (A.K.) was brought to the emergency department of Atmeh Charity Hospital, which is supported by Hand in Hand for Aid and Development and recognized as one of the hospitals accredited for training by the Syrian Board for Medical Specializations (SBOMS). The patient was received by the resident doctor in the specialty of internal medicine, Dr. Abdul Karim Ibrahim.
The patient arrived completely unconscious with wheezing, generalized cyanosis, and massive salivation (froth).
Medical History:
The patient did not have any known medical history, and the parents denied that the girl had been exposed to any toxic or medicinal substance.
Clinical Examination:
The patient’s general condition was very poor, she was unconscious and unresponsive, struggling for breathing, with dilated pupils and pallor, generalized cyanosis, and copious frothing.
- The pulse was threadlike, regular, and rapid.
- Chest: severe groans spread throughout the two arenas
- Abdomen: Soft, breathable
- Extremities: cold, bluish-pale, without edema
Vitalsigns:
- Awareness: Glasgow 6
- Pressure: 80/40
- Pulse: 140
- Oxygen saturation: 88% then began to drop until it reached 47% prior to intubation
Investigations:
- Blood sugar: 180 mg/dl
- ECG: regular sinus tachycardia (no arrhythmias)
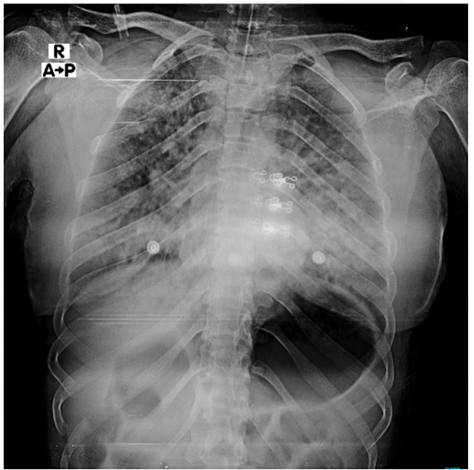
- CXR: Bilateral infiltrates that fill both arenas
- ABG: metabolic acidosis with lactate
Diagnosis:
The initial investigations were directed at a case of pesticide poisoning, and the decision was made to immediately intubate the patient in the emergency department because of her severe respiratory failure, with oxygen support at the highest available concentration and frequent aspiration of her copious bronchial secretions.
Two intravenous lines were also opened to support the patient’s circulation and to start the application of atropine (a specific antidote in cases of insecticide poisoning).
Then the patient was admitted to the intensive care unit and connected to mechanical ventilation, with the completion of the application of atropine and aspiration of secretions.

Follow-up:
The patient’s oxygen saturation began to improve, bronchial secretions dried up, and miosis improved after applying 20 ampoules of atropine. Then the patient began to show signs of awakening. She was weaned off the mechanical ventilator several hours after admission.
After investigation , the patient admitted that she had taken the pesticide with the intention of committing suicide.
The patient stayed for several days in the intensive care unit for the management of aspiration pneumonia, which developed as a result of inhalation of secretions, and she was discharged after 5 days in good health.
Discussion :
Cases of poisoning with pesticides are among the common cases that visit emergency departments periodically. The severity of these cases varies from mild symptoms such as headache, nausea, vomiting, and tearing to severe life-threatening cases. The patient must be evaluated immediately upon his arrival in the emergency department and start managing him directly, by:
- Clearing the airways, supporting circulation, oxygenation, and aspiration of secretions.
- .Support with oxygen at the highest concentration available.
- Initial disinfection of the patient, which includes removing clothing and washing the skin with soap and water.
- There is no benefit from gastric lavage, activated charcoal, or urine alkalization.
- Continuous monitoring of vital signs, heart rate, rhythm, and oxygenation.
- When intubating, Atracurium should be used, and succinylcholine should be avoided.
- If the patient develops seizures, they are treated with benzodiazepines, and phenytoin is avoided.
- The cornerstone of management is the administration of high-dose atropine 1-2 mg intravenously in adults repeated every 5 minutes until bronchial secretions dry up.
- Pralidoxime is given in a dose of 1-2 g to adults mixed with normal saline and given as an intravenous infusion over 5 to 10 minutes.