

Patient history:
A 68-year-old patient arrived at the ER department of Al-Quds Hospital, supported by the Hand in Hand Relief Organization, with a story of abdominal pain about 6 hours ago. The patient described the pain as continuous and increasing in intensity. He was received by Dr. Mustafa Al-Armali, a third-year internal medicine resident. Dr. Mustafa took a detailed medical history from the patient and the patient did not have any previous history of disease or smoking history. The patient described the pain as the worst in his life, the pain began around the navel sharply and increasingly did not respond to painkillers at home.
Clinical examination:
The examination was pale, arterial pressure 110/70 mm g, pulse 120 / min, and oxygen saturation 98%. The patient had acute abdomen pain with a muscular defense accompanied by palpation of a pulsating mass on the median line. Under the supervision of Dr. Wassim Zakaria, a specialist in internal medicine supervising the hospital, an abdominal echo was performed. The echography showed the presence of an abdominal aortic aneurysm. Then a CT abdominal with vascular contrast was done which detected a massive abdominal aortic aneurysm measuring 11 cm with suspicion of rupture and hematoma behind the peritoneum.

Management:
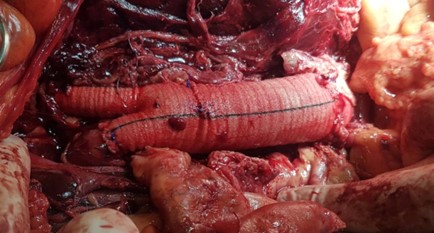
The patient was placed on schematic monitoring and saline serum was given before and after the administration of the contrast substance in order to preserve renal function from damage due to advanced age and to maintain arterial pressure appropriately. An online vascular surgery consultation was then performed, and the decision was the indication of ambulatory surgery. Coordination was made with the Department of Vascular Surgery at Maarat Misrin Hospital, supported by the Syrian American Medical Society (SAMS), so the patient was sent with recommendations to maintain hemodynamic stability during the transfer process, which took about 3 hours due to the dense fog on the road. In Maarat Misrin Hospital the vascular surgery team consisting of a third-year vascular surgery evaluator, Dr. Muhammad Basel Staif, and Dr. Mohamed Al-Sheikh, were waiting for the case. After the evaluation was carried out, the patient developed a stabbing pain, most severe in the back with the development of shock signs. The patient arrived with arterial pressure of 70/50 mm g, with a rapid pulse and a decrease in oxygen saturation, the decision was to do an urgent surgical intervention and blood and plasma transfusion according to recent recommendations. The abdomen was opened, the neck of the aortic aneurysm was clamped, bleeding was controlled, then the aneurysm was opened and the aortic pants were implanted.
The surgery lasted about 6 hours, then doctors sent the patient to intensive care, and he was placed on ventilation for 24 hours, then weaned from the ventilator. The clinical evaluation of the patient showed that the perfusion returned to the lower extremities and the abdominal pain diminished. The laboratory evaluation became within normal 48 hours after admission to the intensive care unit. The patient was discharged to the ward in good health for four days and then discharged home in good health.
Discussion:
Abdominal aortic aneurysm (AAA), is a localized destination more than 50% larger than the normal diameter of the artery. The aneurysm is a common but potentially fatal condition. . The aortic aneurysm ruptures in approximately 50% of patients who arrive at the hospital for treatment, and between 30% and 50% may die in the hospital despite significant advances in intensive care and surgical techniques.
An abdominal aortic aneurysm is seen four to six times more commonly in males than in females, but females suffer more rupture than men. The main risk factors for the development of abdominal aortic blood include:
- Aging
- Male sex
- Ethnicity the white
- Family history
- Smoking
- Presence of another aneurysm in large blood vessels
- Risk factors for atherosclerosis.
Although diabetes is a strong risk factor for atherosclerosis, it is negatively associated with the development of aneurysms. Multiple factors affect aortic dilatation and risk of rupture, the most important of which is the aortic diameter and constant smoking.
Most patients with abdominal aortic aneurysms do not experience any symptoms. They are usually detected by chance due to a routine examination or during imaging studies to assess unrelated suspicion.
Aneurysm symptoms can sometimes occur if the aortic aneurysm expands rapidly, becomes large enough to compress surrounding structures or when ruptures. Patients often experience abdominal, back, or flank pain as in our patient, which may or may not is related to a rupture of the blood. In about 50% of patients with rupture, there is the classic triad: acute abdominal pain, flatulence, and circulatory instability. It can also manifest itself with other clinical manifestations such as limb ischemia (acute or chronic).
The definitive diagnosis requires abdominal imaging studies that show focal dilation of the aorta that meets the criteria for aneurysms > 1.5 times the normal diameter. Abdominal ultrasound and computed tomography of the abdomen are very sensitive, and the ECO is sufficient for evaluation in unstable hemodynamics cases.
Initial management of symptomatic patients (with and without rupture) included intravenous fluid administration, pain relief, and preparation for surgery. For patients with aneurysm rupture, we suggest maintaining systolic blood pressure between 80 and 100 mmHg (permissive hypotension) instead of higher levels before delivery. Permissive hypotension may reduce the persistence of the rupture of the aorta and reduce blood loss.
When a rupture of an aneurysm is diagnosed an emergency repair should be performed to give the patient the best chance of survival. For symptomatic patients (without rupture) it is suggested to repair sooner.
Patients with a rupture of an aneurysm m with a hemodynamic disorder should be transferred directly to the operating room for immediate bleeding control and repair of the aneurysm.
Intravascular repair is considered a preference over open repair as it has been shown to be associated with reduced rates of perioperative morbidity and mortality (30 days).